CASE 30: Revision due to severe adverse reaction to metal debris (ARMD) using a custom 3D printed cup

The Story
“June came to us in 2009 for a revision of her metal-on-metal hip implant. At the revision operation we found 20cm of dead proximal femur, striped of all muscles. We cemented a stem and used a constrained acetabular liner to achieve stability and expected her to return for further surgery within a year. As it happened, she avoided surgery for a further nine years.
On returning to us, we removed June’s dead proximal femur and used a 3D-printed acetabular implant (with constrained and dual mobility liner). The key was to achieve maximum possible fixation to the pelvis in the absence of proximal thigh muscles.”
The Investigation
June was 79 years old when she came back to us in 2018 with swelling in her left thigh.
18 months prior to her referral she had developed swelling in her left thigh with fevers, malaise and night sweats. This was on the background of a left total hip replacement. DVT and malignancy were excluded. A CT scan showed a large collection around the left hip and a raised inflammatory marker: CRP = 198 mg/L (normal is less than 10).
Sepsis surrounding her left THR was suspected and she underwent a washout procedure at her local hospital. Samples grew pseudomonas aeruginosa so she was discharged on meropenem and referred to our clinic.
The Evidence


Anteroposterior plain radiograph showing scalloping on the lateral aspect of the left proximal femur. Lytic areas are evident surrounding the cement mantle of the Exeter stem. The acetabular component has a constrained liner.
The Diagnosis
June’s case and imaging were reviewed by the infection Multi-Disciplinary Team (MDT). They diagnosed an infected left total hip replacement with massive soft tissue destruction. The challenge was to achieve a stable hip, free of infection and without dislocation (despite severe destruction of all proximal thigh muscles).
The Plan
The decision was made to treat her pseudomonas infection with a two-stage procedure.
The First Operation
The first stage was to remove the old metal work, implant a proximal femoral spacer and treat the infection with an antibiotic regimen of meropenem, amikacin and teicoplanin.
This first procedure was done in conjunction with vascular surgeon, Alex Loh, to protect the femoral vessels which were adjacent to the massive soft tissue mass.
The First Outcome



Anteroposterior and lateral plain radiographs demonstrate the new proximal femoral spacer in situ.































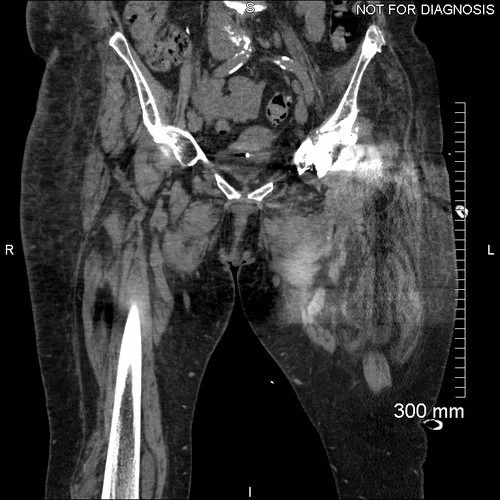





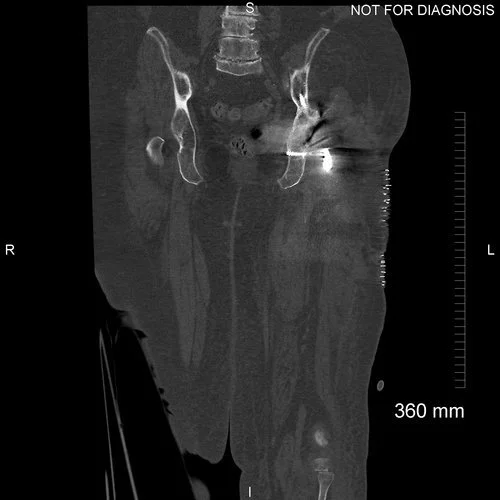
Coronal CT scan taken to plan for the custom acetabular component
Two days after the operation this construct dislocated – probably because of the lack of proximal thigh muscles. June was walking at home with a Zimmer frame when she felt a pop in her left hip. She wasn’t in any severe pain but she was uncomfortable.
The Second Operation
A girdlestone procedure was completed and a skeletal traction pin implanted. We removed the dislocated spacer with ease and removed the proximal cement from the femur.
The surgical site was washed with saline and aqueous chlorhexidine and we carried out a debridement of the membranous layers.
4g of vancomycin and 1g of gentamicin were instilled in Stimulan beads. Finally, a skeletal traction pin was inserted into the distal femur.
The Second Outcome

Anteroposterior plain radiograph demonstrating the girdlestone joint with surrounding antibiotic beads.
The Third Operation
Stage two was carried out 11 weeks after the girdlestone procedure. A proximal femoral replacement and a custom 3D-printed trabecular titanium acetabular component were implanted.




3D CT reconstruction showing the hemipelvic defect



Implant design showing the custom acetabular implant designed around this patients bony anatomy. The blue areas highlight regions of trabecular titanium.
The Third Outcome



Anteroposterior and lateral plain radiographs showing good bony contact surrounding the acetabular component. All of the screws are optimally positioned. The proximal femoral replacement is now in situ.









































Coronal CT scan demonstrating optimal positioning of the acetabular component.
Six weeks after the operation, June’s wound had healed well, with a small non-discharging sinus present. Her inflammatory markers had reduced to a CRP of 27. On clinical examination of the joint, there was no pain on internal or external rotation. June was able to walk with the use of a walking frame.
At her two-month review, June no longer needed to use the Zimmer frame and could walk with the help of two crutches. The CRP remained stable.


Anteroposterior and lateral plain radiographs taken 7-months after June’s operation. There is no evidence of either acetabular or femoral component migration. June remained very happy with her level of function.
12 months after the operation she was still walking and had a satisfactory plain radiograph with no sign of loosening.
The Verdict
“June showed massive soft tissue destruction due to a previous metal debris inflammatory reaction. Further revision risked instability and she managed to cope without 20cm of proximal femur and skeletal traction for three months before her definitive operation.
Extreme soft tissue instability requires very good acetabular fixation, which can be more easily achieved with a custom-made implant.”
-
-
Please see Case 31
-