CASE 32: Revision for infection using a non-modular long femoral stem

The Story
“Bill is an octogenarian who was struggling with an oozing right hip wound. He’d had revision surgery two years previously due to a bad reaction to metal debris from his ASR metal-on-metal hip – but his wound had never fully healed and he was in a lot of pain. What’s more, he had to control the oozing with a colostomy bag.
Knowing he was in need of another operation, I wanted to avoid a big revision that would prolong Bill’s recovery time and result in more bone loss. The challenge, therefore, was to remove the well-fixed stem without having to cut the patient’s thigh bone.”
The Investigation
Bill presented to the clinic with worsening stiffness, pain and significant oozing of the right hip, which required a colostomy bag.
In 2007, he’d had bilateral ASR XL metal-on- metal hip replacements, which were revised nine years later due to raising blood metal ion levels.
On examination:
He was mobile with the use of a walking stick.
He was Trendelenburg-negative on both sides.
He had reduced ROM in the right side due to pain.
He had intact foot pulses and sensation.
Our investigations showed that his blood inflammatory markers were raised (CRP = 63mg/L) and the aspiration from his right hip tested positive for Enterococcus andStaphylococcus lugdunensis. A two-stage procedure was recommended by the bone infection MDT.
We requested an MRI pelvis to assess soft tissue changes (see below).
A CT scan of the pelvis showed there was adequate bone stock present in the pelvic and femoral bone.
The Evidence

Anteroposterior plain radiograph showing a well-fixed right hip replacement.


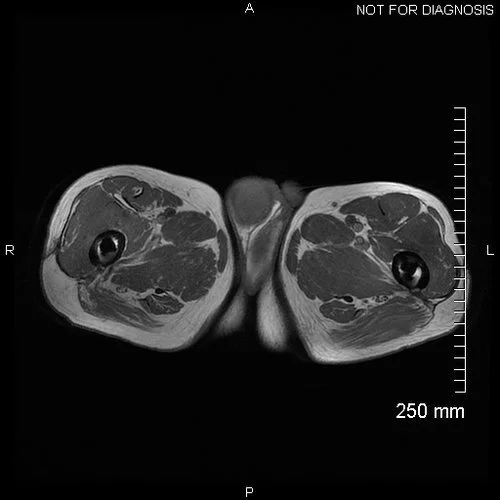


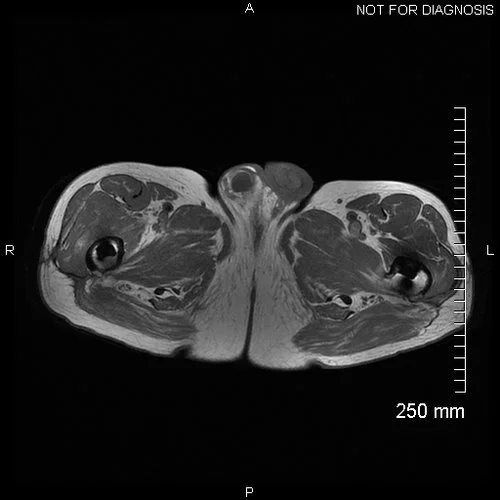

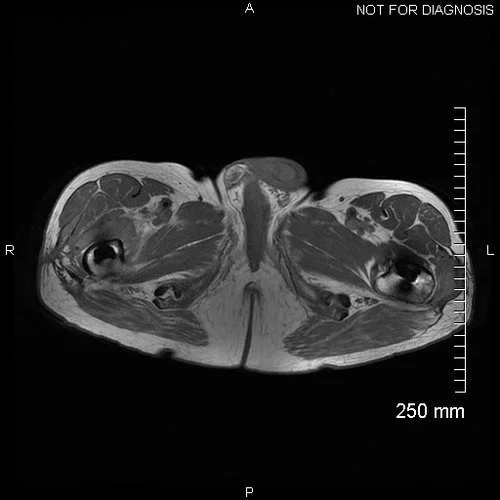





















Axial MRI showing significant fluid collections around both hips, with considerable abductor muscle destruction. The fluid collection around the right hip extends to the wound.



































Coronal CT showing good remaining bone stock in the pelvis.
The Diagnosis
Bill’s right hip replacement was infected with Enterococcus and Staphylococcus lugdunensis bacteria. He was also suffering with damage to his main walking muscles around the hip (the abductors) due to an adverse reaction to metal debris from his previous ASR metal-on-metal hip.
The Plan
Bill required a two-stage operation in order to treat the infection. An infection with Enterococcus and Staphylococcus lugdunensis cannot be treated by antibiotics alone; the metal work has to be removed first.
Stage One:
Plan A was to extract the well-fixed stem without an osteotomy, using a Midas Rex pencil reamer, flexible osteotomes and a Corail stem extractor. This procedure would help the patient make a quicker recovery.
Plan B involved removing the stem through an extended trochanteric osteotomy with the use of three cerclage cables and long stem spacer.
Stage Two:
We would remove the spacer and implant a definitive hip replacement with a design that was appropriate for the plan we had followed.

Pre-operative 3D reconstructed CT of the patient’s anatomy and implants. Image courtesy of LEXI Co., Ltd.

3D plan of the acetabular and femoral components’ position and orientation (blue and red respectively, right side). Image courtesy of LEXI Co., Ltd.
The Operation
For the first-stage operation, we used a posterior approach to the hip and the scar and sinus were excised. Like all revision hip operations, we take five samples of the capsule to send to microbiology.
We approached the well-fixed stem from the top, setting ourselves a time limit of 15 minutes to achieve Plan A. The deadline was random, but it’s sensible to limit this stage and opt for osteotomy if needed. Fortunately, in Bill’s case, it wasn’t.
Using a Midas Rex pencil reamer, flexible oseotomes and a Corail stem extractor, we removed the stem without damage to the proximal femur. The acetabular component was removed with an explant device which has sharp, curved blades and a centrering device.
We washed the surgical site thoroughly with Savlon and saline before making the antibiotic impregnated cement. For this case, we used a combination of vancomycin and gentamicin in the cement. We then implanted the C-stem femoral spacer with a metal head and a polyethylene liner. We completed our intraoperative check for stability and leg length, and finished by closing layers.
Eight weeks later, after systemic and local antibiotics, we carried out a second-stage hip revision. We achieved exposure of the surgical site through the old incision and removed the spacer.
Once again, we sent five samples of capsule to microbiology to assess for successful treatment of the underlying infection. Despite two previous hip replacements, there was adequate bone stock to ream the acetabular socket to 64mm. We needed three screws to achieve optimum fixation.
We rasped the femoral canal to 14mm and implanted a long stem Corail. We opted for a ceramic head and a polyethylene liner in this patient. Leg length and stability were once more assessed before the surgical site was washed and closed.
The Outcome


Anteroposterior and lateral plain radiographs taken after Stage One, demonstrating the cemented C-stem spacer in situ. The stem is very loosely cemented, enabling easy removal at the second stage, but was stable enough for walking with two crutches and avoiding dislocation during the inter-stage period.


Anteroposterior and lateral plain radiographs taken six weeks after Stage Two demonstrates optimum positioning of the new Corail stem and the acetabular shell.
At three weeks post-op, Bill was able to walk up to three quarters of a mile with the help of crutches. The wound had healed and it was no longer oozing. One year on, Bill was delighted with his revised right hip, and the examination and radiograph were highly satisfactory. Plan A had proved a great success.
The Verdict
“Component removal is necessary to treat an infected hip replacement like Bill’s. For explanting a femoral stem, I suggest the following two plans:
Plan A: Remove the stem from the top without osteotomy.
Tools: Midas Rex pencil reamer (it’s more effective than k wires, but beware ease of exiting the femur); flexible osteotomes; extractor with slap hammer.
Plan B: Perform an extended trochanteric osteotomy.
Tools: Use standard saw, then reciprocating saw, then midas rex for distal corners, then two large osteotomes to lever open the bone. You’ll need three cables and a trochanteric plate may be required.
Ideally, well-fixed components are removed by following Plan A. By avoiding damage to the bone, you’re minismising complexity and also the final implant size.
Without the significant bleeding, healing and long recovery time associated with Plan B, patients like Bill can get back to enjoying their lives much sooner – and with more of their bone stock intact.”
-
-
-
https://www.complexhipsurgery.com/femoral-stem-extraction-case-one