CASE 16: Proximal femoral replacement and a custom 3D-printed acetabulum, for severe adverse reaction to metal debris

The Story
“A 76 year old female presented with a painful, dislocating, shortened and infected right proximal femoral replacement after having undergone 25 right hip operations.
In 2008 she had a right total metal-on-metal hip resurfacing. She developed ARMD which required multiple operations for debridement. She then developed an infected hip. One of her inpatient stays was for 365 days, during which she had 15 operations.
One of her operations was for a vertical rectus abdominis myocutaneous (VRAM) flap to cover her soft tissue defect.”
The Investigation
Examination revealed that she was chair-bound and unable to walk. She transferred with the aid of a leg calliper due to her sciatic nerve palsy.
Blood tests revealed an ESR of 26mm/H and a CRP of 19mg/L.
The Evidence


Above there are two anteroposterior (AP) radiographs of the patients pelvis. The top image shows a located proximal femoral replacement in a custom trial-flange-flange acetabulum.
The bottom image shows that this has dislocated due to instability, causing the patient pain.

Above is a pre-operative long leg film. Note that there is a 4.5cm block under the right foot.
The Diagnosis
This patient was diagnosed with a painful, dislocating, shortened and infected right proximal femoral replacement.
The Operation - Stage One
The plan was for a two stage revision for her right hip.
She underwent first stage revision surgery in July 2016. An articulating spacer was not used because of the soft tissue destruction. Imaging after the first stage provided good quality CT images to plan and make a custom made acetabular implant. This implant was chosen to maximise the fixation so that a constrained liner with dual mobility articulation was possible whilst minimising the risk of implant loosening.
Samples from the first stage surgery grew Pseudomonas and Proteus. The patient received a 6 week course of Cefazidimine and her CRP at the end of this was 11mg/L. The sinus however was still discharging.
The patient was discussed at the Bone Infection MDT at the Royal National Orthopaedic Hospital and the decision was made to repeat the first stage of the revision.
The Outcome - Stage One

Anteroposterior radiograph of the pelvis from September 2016. The metal work has been removed on the right side.



























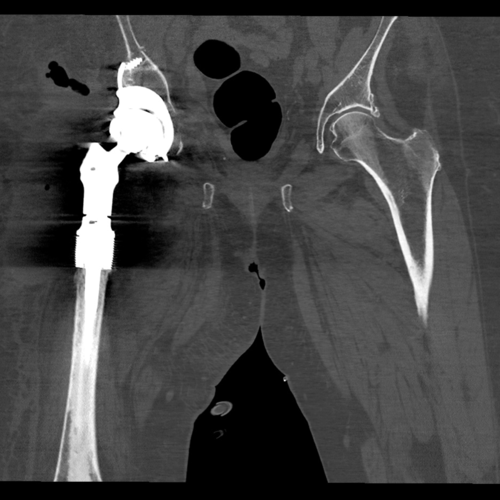
This CT was used to design and plan the acetabular component of this revision surgery. It was also used in the planning of the proximal femoral replacement.

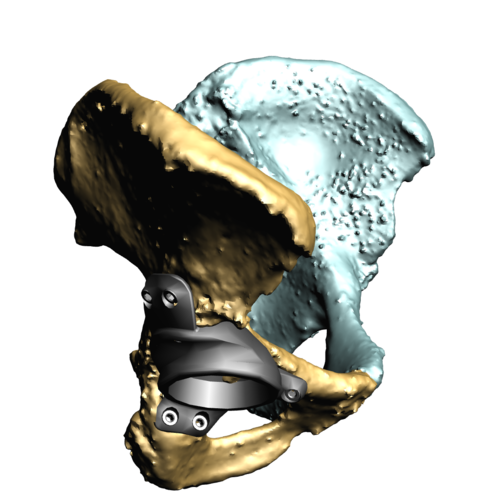
This 3D model of the patient’s right hemipelvis has been recreated from the post-operative first stage computer tomography scan demonstrating a Paprosky 3B pelvic defect.
The Operation - Stage Two
METS Proximal Femoral Replacement
Acetabular Implant Design
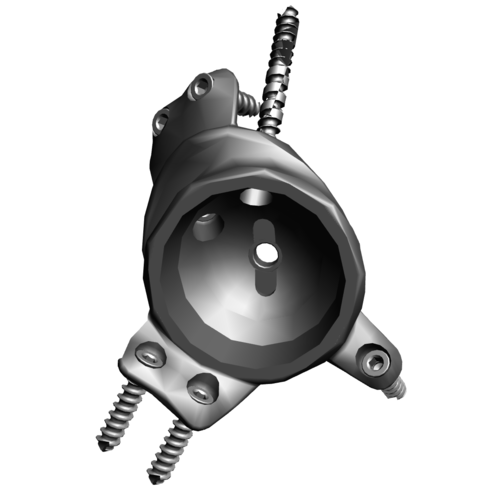
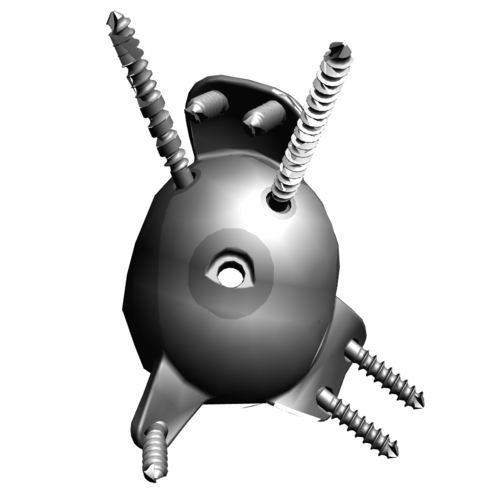

This shows a 3D representation of the custom acetabular component. It is made using trabecular titanium which encourages bony ingrowth into the implant. Look at acetabular case 8 for more information.

The METS proximal femoral replacement system is a modular proximal femoral replacement with a cemented stem and HA collar to achieve initial stability and encourage bony ingrowth.
The patient underwent 2nd stage revision surgery with a custom made, 3D printed titanium acetabular and proximal femoral replacement. She was delighted at being able to transfer and take some steps.
The Outcome - Stage Two


Radiographs - these radiographs are from 6 months after the operation showing the METS proximal femoral replacement articulating with the custom Trabecular Titanium acetabular implant. Both components are well fixed and well positioned.

3D Reconstruction
This is a computer generated 3D reconstruction of the proximal femoral replacement and custom acetabular implant in situ, produced from the post-operative computer tomography scan.











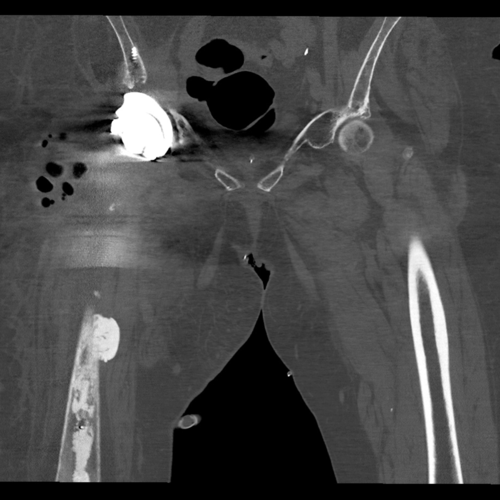



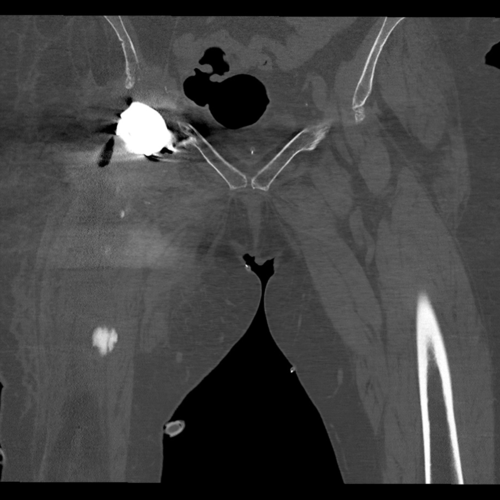

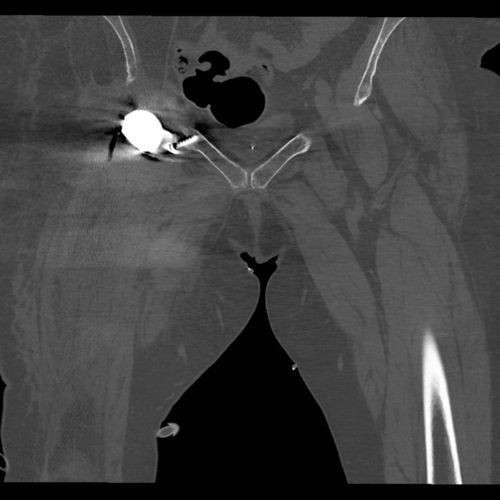
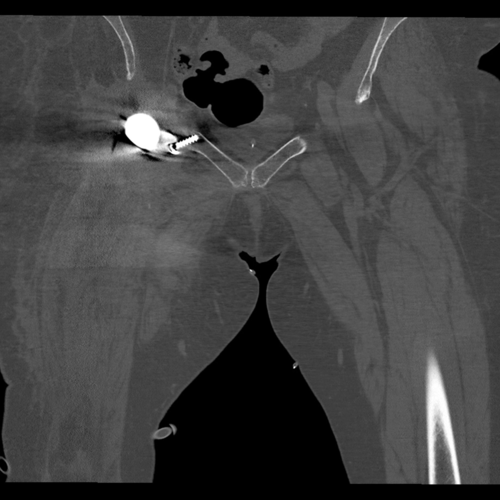
CT scan - scroll through the post-operative computer tomography scan. This shows the acetabular component with good contact to the host bone and a well-positioned proximal femoral replacement.

Post-Op EOS Scan
This is a full body post operative EOS scan which demonstrates the standing functional position of the implant.
The Verdict
“The patient was delighted at being able to transfer from bed to chair comfortably: the first time in 5 years. She was able to walk with two crutches across the clinic room. She had no pressure sores.
The Infection was still ongoing at this point.
ARMD and infection is one of the hardest hip problems to resolve.
Custom made acetabular implants increase the chance of implant fixation when there is high stress due to a constrained liner and several soft tissue destruction.”